














 218-219 / 568
218-219 / 568

Automatic Detection of Pain in Finger Amputees
Stump pain and phantom limb pain (PLP) are commonly felt in the part of a limb that
remains after an amputation. The etiology and pathophysiology of PLP are poorly
understood and has been studied by a lot of researchers. However, none of those
seem to investigate the ability to recognize pain in an amputated finger.
Hedi Adamov, Noa Shprach
Advisor: Dr. Anat Ratnovesky, Dr. Gabi Shafat
Medical Engineering
Classification: The classification was carried out in two ways, binary and multiclass
classification and were evaluated using stratified 5-folds cross validation method. The
classifiers that were used are KNN, SVM, decision tree and a majority decision
(selecting the class that appears most often by the classifiers). The evaluation metrics
that were used are accuracy, precision, recall and F1-score.
High prediction rates were achieved for the binary classification and satisfactory
rates for the multiclass classification.
The highest success rates were obtained using the decision tree classifier and
feature selection.
Good recognition rates were achieved using the PPG sensor alone, demonstrating
that the PPG holds a major part in classifying pain levels.
Integrating multiple biomedical signals with machine learning methods proved as a
reliable approach for finger amputation pain recognition.
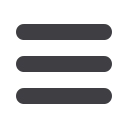
The experimental system was designed to record
physiological signals of skin temperature, skin
conductance and blood volume changes, using
Arduino, 5 switch buttons (for pain level) and three
sensors, NTC, GSR and PPG. The experimental
protocol includes simultaneous measurements of the
signals, recorded after activities in order to stimulate
pain in the finger. During each session, the subject
reported his pain level.
1. Introduction
2. Objective
3. Methods
To develop a pain assessment algorithm for patients suffering from pain after a finger
amputation based on physiological signals acquired by three sensors: NTC-thermistor,
galvanic skin response (GSR) and photo-plethysmography (PPG).
3.1. Experiment apparatus and Protocol
3. Results
Feature extraction: New vectors were calculated from the original signals: heart rate
(HR) and Peak-to-Peak (PP) from the PPG signal and changes in skin temperature (dT)
from the NTC signal. Later, statistical features such as mean, standard deviation and
variance were extracted from the vectors to create the final dataset that contains 30
features.
Dimension Reduction and Feature Selection: The data was classified using all
features, features selection (based on variance threshold) and dimension reduction to a
third of the features using PCA. Each of these methods were examined with different
number of sensors.
4. Discussion
Figure 2. Experimental apparatus
Figure 1. Amputated finger
(a)
(c)
(b)
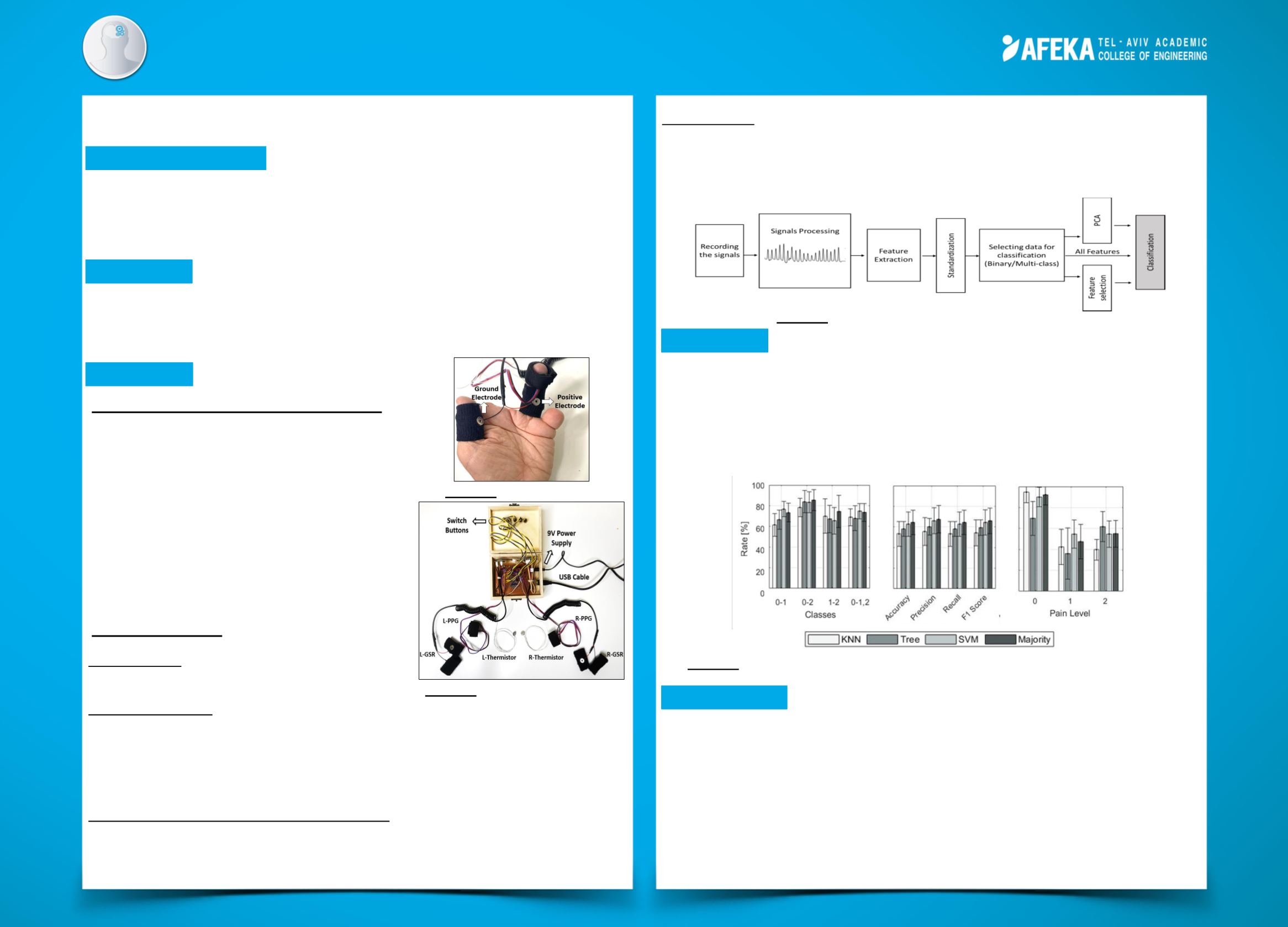
For binary classification, the highest accuracy rates when classifying between class
0 vs 1, 0 vs 2, 1 vs 2 and 0 vs 1&2 were 82.8±8.0%, 87.3±7.3%, 74.3±15.6% and
82.3±4.9%, respectively.
For multiclass classification, the highest accuracy rate was 64.9±5.9% while the
recall rates for classes 0, 1 and 2 were 94.7±10.2%, 54.2±15.4% and 67.2±17.5%,
respectively.
Figure 4. Evaluation of: (a) binary classification, (b) multiclass classification and (c)
recall rates of each class in multiclass classification
Figure 3. Schematic structure of the pain recognition
system
3.2. Data Analysis
Segmentation: The signals were segmented
according to the pain levels reported.